Learning Objectives
- Describe the major anatomical features of the vertebral column including its innervation; and vertebral and intervertebral anatomy.
- Outline the physical exam to conduct with a patient complaining of back pain.
- Compare and contrast the most common causes of back pain.
- Compare and contrast the use of MRI and X-rays, and explain why MRI is used for diagnosing this patient.
- Describe the mechanisms of action and contraindications of ibuprofen and acetaminophen.
- Explain the roles of physical therapists in treating patients.
- Explain the prognosis and treatment plans for a herniated nucleus pulposus and sciatica.
Case Summary
Jane is a 42-year-old woman who presents with back pain radiating to the left leg that began from bending over following a long brisk walk. Jane had recently begun training to walk the Susan G. Komen Race for the Cure after being sedentary for years. Acetaminophen has not helped her over the weekend, so she sees her doctor Carolyn Kim. Dr. Kim advises ibuprofen and watchful waiting. Several days later, Jane further injures herself with a stairstep misstep in the dark. The next morning, she returns to Dr. Kim with increased pain in her lower back and even more so in her leg. Because the condition has worsened, MRIs and prescription strength ibuprofen are ordered. The MRIs show disc herniation between L5 and S1. Over the next month, Jane does physical therapy and takes ibuprofen as prescribed for pain. At the end of the month ibuprofen is no longer needed as the symptoms subside.
The case centers on the anatomy of the lower spine and lower extremity. Pharmacology concepts include the mechanism of action of the NSAID ibuprofen, and comparing and contrasting the mechanisms of action of ibuprofen and acetaminophen. The case involves an interprofessional interaction between physician and physical therapist. There is a largely normal history taking and physical exam that are intended to be an appropriate introduction to those facets of medicine in a first case for case based learning.
Learning Objectives point by point
Objective 1. Describe the major anatomical features of the vertebral column including its innervation; and vertebral and intervertebral anatomy.
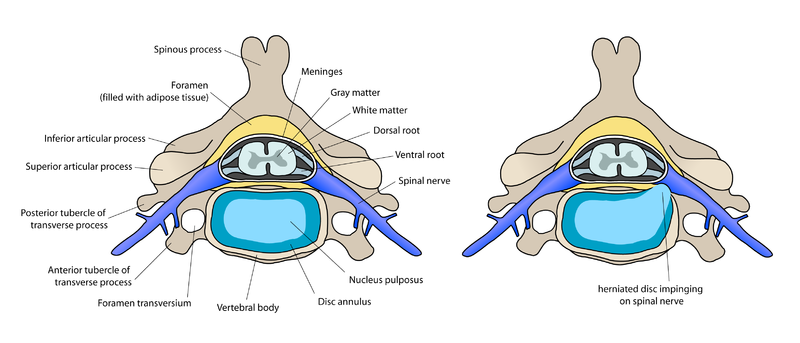
In a nutshell: The 33 total vertebrae are designated as cervical, thoracic, lumbar, and sacral. There are five lumbar L1 to L5 (from head to toe), and below them five sacral S1 to S5. There are cushioning discs between each vertebrae. Each intervertebral disc is composed of the inner nucleus pulposus and outer annulus fibrosus. Herniation of nucleus pulposus is an extrusion of the nucleus pulposus causing the disc to protrude beyond its normal space between the vertebrae.
The 33 total vertebrae are designated as cervical, thoracic, lumbar, sacral, and coccygeal. The 24 cervical, thoracic, and lumbar vertebrae are articulating and the remaining 9 are fused to comprise the sacrum and coccyx. There are five lumbar L1 to L5 (from head to toe), and below them five sacral S1 to S5. There are cushioning discs between each vertebrae. Each intervertebral disc is composed of the inner nucleus pulposus and outer annulus fibrosus. Herniation of nucleus pulposus is an extrusion of the nucleus pulposus causing the disc to protrude beyond its normal space between the vertebrae.
 Henry Vandyke Carter, Public domain, via Wikimedia Commons
Henry Vandyke Carter, Public domain, via Wikimedia Commons
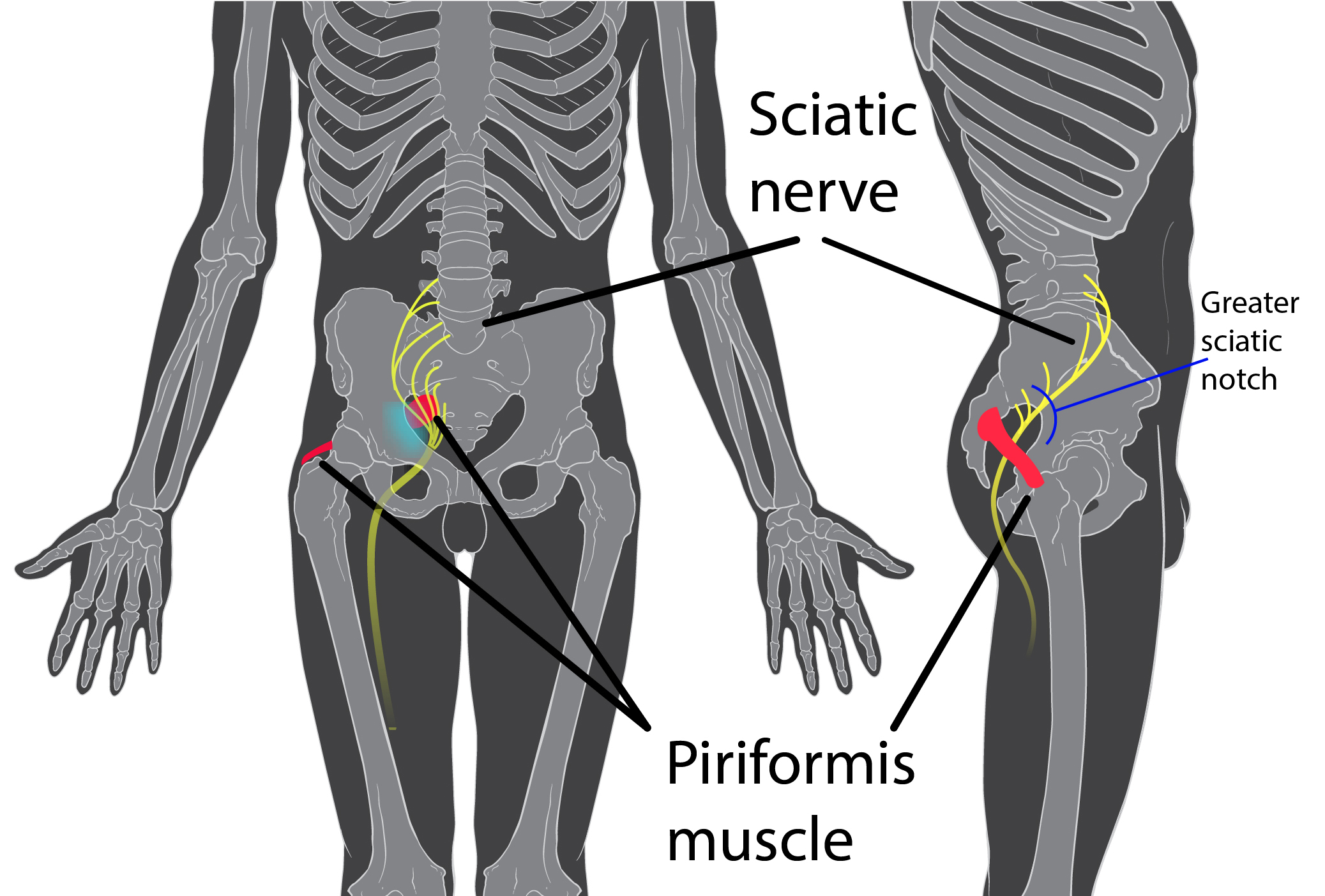
A spinal nerve can be compressed in a number of ways, from a muscle the nerve travels through trapping the nerve, to a herniated nucleus pulposus pinching the nerve where it passes by.
 Patrick J. Lynch & KDS4444
Patrick J. Lynch & KDS4444,
CC BY-SA 2.5, via Wikimedia Commons
 user:debivort
user:debivort,
CC BY-SA 3.0, via Wikimedia Commons
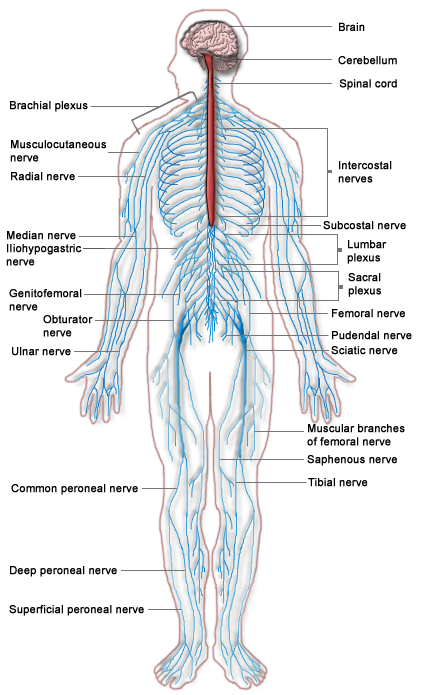
Nerves run through the vertebral column and into various specific regions of the lower extremity as shown above. The lumbosacral plexus is composed of spinal nerve segments L4–S4. It gives rise to the three major peripheral nerves of the lower extremity: the femoral nerve (L2-L4 innervates the anterior compartment of the thigh), the obturator nerve (L2-L4 innervating the medial compartment of the thigh), and the sciatic nerve (L4-S3 innervates the posterior thigh, leg (anterior/lateral/posterior), and foot. The sciatic nerve, by far the largest of the three, divides into the tibial and common fibular (peroneal) nerves. If the sciatic nerve is pinched at the spine, the patient will feel pain in the parts of the body innervated by the nerve, in this case the buttocks and posterior upper leg on one side.
Please see the spinal nerves as shown in the diagram below. The sciatic nerve is easily seen near the middle of the diagram noted in the right column of nerve names.
¤~Persian Poet Gal, Public domain, via Wikimedia Commons
Objective 2. Outline the physical exam to conduct with a patient complaining of back pain.
In a nutshell: In this case which will be the first patient case the students see, the physical exam is entirely benign with the exception of findings specifically related to the herniated nucleus pulposus with sciatica.
The pain is recent in origin and sudden in onset. It seemed to stem from the bending, leading one to lean away from some otherwise reasonable diagnoses such as tumors in or around the spine, infections such as Zoster sine herpete, or endometriosis. The pain is severe since such things as acetaminophen and heat did not seem to impact it.
The only contributing factor seems to be a change in activity level- having been sedentary and now starting vigorous activity. Her medical, family and social histories revealed no pertinent facts. It is important to recognize that each step of taking and/or updating a history can elucidate clues to the nature of the difficulty experienced by a patient. The students should recognize the different sections of the history after completing this part.
The physical exam is entirely benign with the exception of findings specifically related to the herniated nucleus pulposus with sciatica. Lower back muscle strain would be unlikely to be associated with the buttocks pain, and particularly not with the leg pain. The pain would be felt only in the region including and surrounding the muscle. A tumor will be detected by imaging by x-radiography or MRI. Typically, a tumor will cause unremitting pain that grows steadily and is unaffected by activity or position, although these characteristics are too variable between patients to be reliable for use in diagnosis.
The relevant part of the exam was the specific deficits seen involving the left leg, the leg in pain. Strength testing is done on a five-point scale, where a 5/5 indicates best expected function, and 0/5 indicates paralysis. The best expected strength 5/5 would of course differ between a professional football player and a grandmother.
Deep tendon reflex tests are one means to attempt to localize a problem that is neurological in origin. This generally entails tapping a portion of the body with a small hammer that has a rubber head, known as a reflex hammer. For Jane the reflex that is impaired is the Achilles or ankle reflex, observed by tapping Jane over the Achilles tendon and noting the degree to which her foot and leg jerk in response to the tap. In Jane’s case there is a normal amplitude jerk when tapping her right leg, but a diminished response when tapping her left. This may be associated with damage involving the S1 level of the spine. Another example of a deep tendon reflex is the patellar or knee reflex which is done as indication of damage at the L3 or L4 level.
Ralf Stephan (mailto:[email protected]), Public domain, via Wikimedia Commons
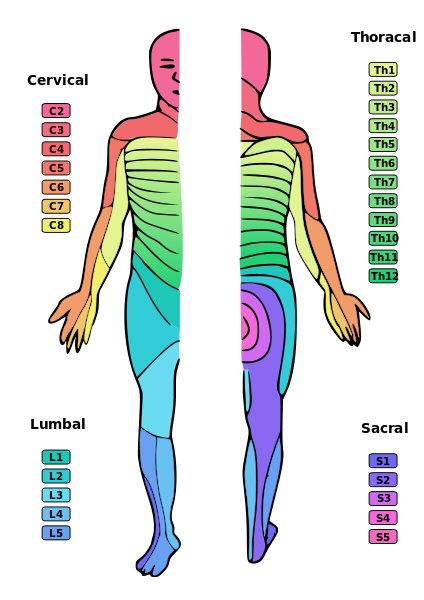
Please recognize the connection between these different vertebral sites of herniation and dermatomes and closely related myotomes.
Symptoms of L5-S1 herniation would include weakness in plantar flexion/toe walking, diminished Achilles reflex, and posterior distribution of pain. Symptoms of L4-L5 herniation would be weakness in dorsal flexion/heel walking, normal reflexes, and lateral distribution of pain. Symptoms of L3-L4 herniation, which is more rare, would be weakness in quads/squatting and rising, diminished patellar reflex, and frontal distribution of pain. Positive straight leg raise is indicative of nerve impingement.
Lower back muscle strain would be unlikely to be associated with the buttocks pain, and particularly not with the leg pain. The pain would be felt only in the region including and surrounding the muscleA tumor will be detected by imaging by x-radiography or MRI. Typically, a tumor will cause unremitting pain that grows steadily and is unaffected by activity or position, although these characteristics are too variable between patients to be reliable for use in diagnosis.
Neither Jane’s description of her onset of pain nor her level of pain cause immediate concern that her problem is more serious. Some of the conditions that might match Jane’s symptoms are indeed quite serious such as spinal or pelvic tumors, or critical nerve damage. Pain may occur when nerves are compressed due to dislocated bone, entrapment by a muscle, or vertebral problems. The sciatic nerve runs through the piriformis muscle, which may also compress the nerve causing pain. Other causes include Zoster sine herpete (shingles without rash) and endometriosis. Certain of these conditions may well require extensive treatment such as surgery.
Lower extremity weakness, saddle numbness, or difficulty with bladder or bowel control indicates the possibility of cauda equina syndrome. This is an emergency situation requiring surgical decompression of the involved nerves. Cauda equina syndrome is an injury of multiple lumbosacral nerve roots within the spinal canal distal to the termination of the spinal cord at L1-L2. The name is derived from Latin, and means horse’s tail in reference to the general location of the impacted nerves at the base of the spine. Immediate MRI imaging followed by surgery is essential for recovery of motor and/or sphincter function. Permanent impairment of these functions can occur, and speedy repair is the best way to avoid permanent impairment.
Objective 3. Compare and contrast the most common causes of back pain.
Common links to back pain include:
- Muscle or ligament strain from continued heavy lifting (made worse by improper form) or awkward movement that puts the back muscles and spinal ligaments under strain
- Bulging or ruptured disks that press on a nerve
- Arthritis
- Skeletal irregularities like scoliosis with an onset of pain at middle age
- Osteoporosis, impacting the cartilage of joints and discs. Spurs result in pressure on nerves of the spinal column
Risk factors for back pain include:
- Getting older (starting around 30-40 years old)
- Sedentary lifestyle – less exercise and weakening of muscles used for supporting posture
- Excess weight putting strain on the back
- Smoking
- Improper form when heavy lifting
- There are links between back pain and psychological conditions such as depression and anxiety
- Various diseases (students may find a variety)
For additional information consult:
Prevalence of chronic low back pain: systematic review.
Meucci RD, Fassa AG, Faria NM. Rev Saude Publica. 2015;49:1. doi: 10.1590/S0034-8910.2015049005874.
Objective 4. Compare and contrast the use of MRI and X-rays, and explain why MRI is used for diagnosing this patient.
In a nutshell: Imaging is not called for in the circumstances surrounding Jane’s initial visit. Sudden worsening of her pain is a reason for the need for imaging. MRI typically does a nice job of showing disc herniation. X-radiography does not, but is done to rule out other dangerous conditions that could be contributing to Jane’s symptoms. In Jane’s case the MRI is done first, and only if the MRI does not show the reason for her pain will an x-ray be necessary.
An MRI or magnetic resonance imaging involves excitation of body organs and tissues by a fluctuating magnetic field such that those with differing magnetic properties are visible and distinct from each other because they activate differently in the field. Different patterns of excitation cause different organs and tissues to show up differently. This all differs from x-rays because x-rays are essentially a shadow thrown onto film due to different organs and tissues (e.g. bone) having different densities for x-rays to pass through (or not be able to pass through).
Imaging is not indicated in acute lower back pain or sciatica. One indication for MRIs and x-rays is sciatica that does not resolve in six weeks. An MRI becomes indicated for Jane when the condition suddenly worsened following the misstep on the stairs. Imaging after symptoms subside is contraindicated. It was done in this case only because Jane was in a research study which included an MRI as part of the study. The physical therapist told her of a study that matched her symptoms, and Jane decided she would like to enroll.
In asymptomatic individuals, about 20% will have findings of disc herniation, and about 30% will show a bulging disc. This lack of specificity of MRI as a tool utilized to diagnose these conditions makes an MRI unsuited to routine diagnostic use for lower back pain problems. There would be an unacceptable number of false positives. The physical exam is adequate for diagnosis except in cases where sciatica lasts 6 weeks, or where pain, numbness, or other indications make an MRI needed. At this point imaging is necessary to see more precisely what the patient’s situation is in the event there is a condition that requires emergency treatment, or the imaging is used to guide surgical intervention decisions.
Imaging by x-ray is also not indicated for acute lower back pain or sciatica. X-rays were done along with the MRI due to the sudden worsening of Jane’s symptoms. X-rays may sometimes show alteration in height of the intervertebral space, but generally do not show disc herniation. Therefore, they are not informative in herniated nuclear pulposus. X-rays for lower back pain are useful to rule out issues other than disc bulging or herniation, issues such as spinal column tumors, neurofibromas, pelvic tumors, pelvic fractures, or spondylolisthesis (displacement of vertebrae out of alignment thereby tugging and compressing the nerve).
Sciatica may also be mimicked by other causes for which imaging is not relevant. The sciatic nerve runs through the piriformis muscle, which may also compress the nerve causing pain. The infectious disease Zoster sine herpete is another nonspinal cause of sciatica, though obviously not visualized by x-radiography.
For additional information consult:
Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians.
Chou R, Qaseem A, Owens DK, Shekelle P; Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2011 Feb 1;154(3):181-9
Objective 5. Explain the courses of action taken by the patient.
In a nutshell: Ibuprofen inhibits the enzyme cyclooxygenase. This enzyme forms signaling molecules for pain and inflammation, and to regulate a number of other processes. Acetaminophen lacks anti-inflammatory activity, and evidence has not shown acetaminophen to be of benefit in herniated nucleus pulposus.
The drug therapeutic goal with respect to this case is to relieve the pain and inflammation that result from the herniated nucleus pulposus. Ibuprofen is an example of an NSAID, a nonsteroidal anti-inflammatory drug, and evidence based medicine tells us that ibuprofen is somewhat useful in the treatment of sciatica from herniated nucleus pulposus. Advil and Motrin are brand names for the drug ibuprofen. Acetaminophen (acetaminophen) has analgesic properties, but lacks anti-inflammatory properties, and the evidence is that acetaminophen has no benefit in acute low back pain. Unlike NSAIDs, which are peripherally acting, acetaminophen is primarily centrally acting.
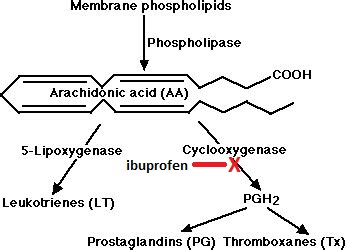
Eicosanoids are signaling molecules that are lipid in nature, thus are limited in mobility and have only local effects. There is a long list of processes eicosanoids regulate, including pain and inflammation (some are signals that promote inflammation, others inhibit it). Other processes regulated by eicosanoids are vascular effects (some regulate vasoconstriction, others regulate vasodilation), bronchial effects (bronchoconstriction and bronchodilation), uterine effects (stimulate contractions when they accompany labor and cramps when they accompany menstruation), renal effects (contribute to blood pressure control), coagulation, erections, fever, and sleep/wake cycle.
The eicosanoids include the prostaglandins, thromboxanes, and leukotrienes. All eicosanoids are made from the fatty acid arachidonate, which is abundant in our diet. There are a number of leukotrienes which are all formed from arachidonate via the enzyme lipoxygenase. There are also a number of prostaglandins and thromboxanes which are formed from arachidonate via the enzyme cyclooxygenase.
The mechanism of action of ibuprofen is to inhibit cyclooxygenases, thereby blocking formation of the prostaglandins and thromboxanes which signal for pain, inflammation and the various processes mentioned above. In this way ibuprofen acts as an analgesic (pain relief) and anti-inflammatory (relief from inflammation).
Ibuprofen and aspirin are two of the many NSAID drugs, and their mechanism is the same. There are isoforms of cyclooxygenase, and ibuprofen and other NSAIDs do not discriminate among them. Cyclooxygenase-1 is constitutively acting, and helps regulate normal processes such as airway function, platelet aggregation, and protection of the gastric mucosa. Cyclooxygenase 2 is induced during injury, responding to inflammation. There are cyclooxygenase-2 specific inhibitors whose purpose is to have an anti-inflammatory effect while at the same time they avoid the adverse gastric effects that occur with cyclooxygenase-1 inhibition. Currently the sole US FDA approved cyclooxygenase-2 specific inhibitor is Celebrex (celecoxib).
The mechanism of action of acetaminophen (acetaminophen) is unknown, but one potential mechanism involves a very specific inhibition of cyclooxygenase such a manner that acetaminophen has the analgesic and antipyretic (fever reduction) actions of NSAIDs, while it lacks their anti-inflammatory and antiplatelet (regulates blood clotting) actions.
Jane was in pain, so she took acetaminophen which she knows is good for pain. It did not alleviate her pain. Acetaminophen is also an antipyretic (reduces fever), an effect that is not relevant in this instance. The pain was so troublesome the patient tried everything she could think of in the way of home remedies.
Mostly Jane bases her expectation that she will feel pain relief from Icy Hot or a heating pad on previous use of the cream and pad, not on her knowledge of the mechanism of action. She of course has a lack of knowledge of how Icy Hot functions. The active ingredients in Icy Hot are menthol and a salicylate. Topical menthol has a transient cooling effect through activating a receptor that is a detector of cold stimuli in sensory neurons known as TRPM8. This cooling effect is accompanied by a pain relief effect. This initial sensation of coolness is followed by warmth and reddening as the topically applied salicylate induces blood flow into the area over which it has been spread. The warmth initiates relaxation which provides pain relief. The menthol and the salicylate also have a counterirritant effect in which their surface irritation masks the underlying pain and discomfort. The heating pad provides pain relief through warmth and relaxation.
For additional information consult:
Non-steroidal anti-inflammatory drugs for sciatica.
Rasmussen-Barr E, Held U, Grooten WJ, Roelofs PD, Koes BW, van Tulder MW, Wertli MM. Cochrane Database Syst Rev. 2016 Oct 15;10(10):CD012382.
Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians.
Qaseem A, Wilt TJ, McLean RM, Forciea MA; Clinical Guidelines Committee of the American College of Physicians, Denberg TD, Barry MJ, Boyd C, Chow RD, Fitterman N, Harris RP, Humphrey LL, Vijan S. Ann Intern Med. 2017 Apr 4;166(7):514-530.
Objective 6. Outline the roles of physical therapists in treating patients.
In a nutshell: The physical therapist is able to work with a patient to instruct and train patients in activities that will help them recover. A physician will typically not have that quantity of time to spend individually with a patient.
This is an example of interprofessional teamwork. The physical therapist has the knowledge, equipment, and time to directly guide the patient through the activities that will most help them. This is precisely what is needed once the physician diagnoses the problem and decides what pharmacological or surgical interventions to implement as well.
The physical therapist will perform a thorough assessment of the patient’s baseline core and back abilities. They can give the patient education about how to protect and strengthen their spine. For example, the patient should avoid positions or movements that hyperextend the spine, for example picking up objects from the floor by rounding the back forward; instead, the physical therapist would recommend getting to ground by bending the knees into a squat position and keeping the back straight. Core stability is important for prevention of pain and reinjury in the future. Therapy includes strengthening the antagonistic abdominal muscles. Examples of exercises include gentle crunches (partial situps), pelvic tilts, and supine knee to chest moves. Hamstring flexibility is also important. Further core stability exercises and flexibility maneuvers such as quadruped flexions can also be taught. After the in-depth evaluation, the physical therapist can tailor the therapies to the individual patient’s strength deficits. As indicated, the physical therapist can assist in these stretches, exercises, and sometimes administer therapeutic massage.
Objective 7. Explain the prognosis and treatment plans for a herniated nucleus pulposus and sciatica.
In a nutshell: Sciatica due to nucleus pulposus herniation is expected to resolve within six weeks even with only ibuprofen therapy. Other treatment modalities such as epidural corticosteroids and surgery are commonly employed.
Fortunately for the patient, sciatica due to herniated nucleus pulposus most often naturally subsides with time. Ibuprofen is valuable as an analgesic during that time. Other interventions are associated with faster progress, but over time conservative treatment with ibuprofen typically yields the same end result.
The doctor and physical therapist should aid in setting goals and limits on activities the patient undertakes to aid in recovery. Aerobic exercise as tolerated is helpful, but must initially be low impact such as treadmill walking and stationary cycling, then working up to swimming or walking. Yoga is ideal as well, and can be continued long after symptoms subside. There is evidence also that mindfulness-based stress reduction and superficial heat are of moderate benefit. A Cochrane review of the literature found no benefit of manipulative therapy on acute low back pain, whether delivered by chiropractors, manual therapists, or osteopaths.
Epidural delivery of corticosteroids is one treatment that has been shown to be effective in faster resolution of pain and quicker regain of function. Long-term, however, studies show conservative treatment equals epidural steroids for benefit. Particularly when the condition is not much improved within six weeks, surgery may also be an option, though obviously far more invasive. Microscopic diskectomy and laminectomy with surgical removal of herniated material are usually the procedures of choice. Certain of these procedures may be done in a minimally invasive manner, making them more tolerable. Even with surgery, success in terms of freedom from pain and fully regained function are many times not achieved.
For additional information consult:
Diagnosis and treatment of sciatica.
Jensen RK, Kongsted A, Kjaer P, Koes B. BMJ. 2019 Nov 19;367:l6273.
Spinal manipulative therapy for acute low-back pain.
Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW. Cochrane Database Syst Rev. 2012 Sep 12;(9)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Ralf Stephan (mailto:[email protected])](https://commons.wikimedia.org/wiki/File:Dermatoms.svg){kind=link}